Recommendation 1.2.2.1 We recommend using eGFRcr-cys in clinical situations when eGFRcr is less accurate and GFR affects clinical decision-making (1C).
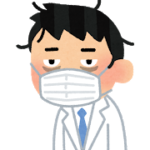
Recommendation 3.4.1 We suggest that adults with high BP and CKD be treated with a target systolic blood pressure (SBP) of <120 mm Hg, when tolerated, using standardized office BP measurement (2B).
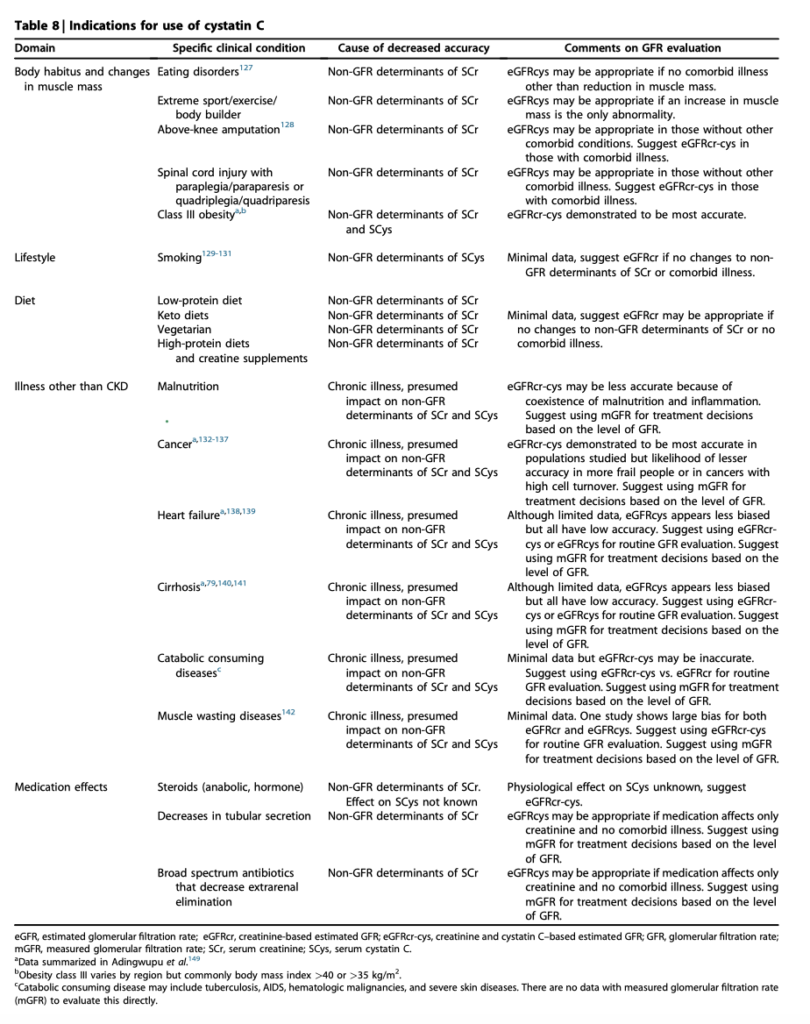
Practice Point 3.6.3: Hyperkalemia associated with use of RASi can often be managed by measures to reduce the serum potassium levels rather than decreasing the dose or stopping RASi.
Practice Point 3.6.7: Continue ACEi or ARB in people with CKD even when the eGFR falls below 30 ml/min per 1.73m2
Resource use and costs. Health economic analyses are required in people with CKD without diabetes and low levels of albuminuria to establish their level of cost-effectiveness. From a healthcare system perspective, reducing the cost burden of hospitalizations and dialysis is highly desirable, and QoL may be preserved longer from their avoidance. Specifics as to whether people bear the costs of these medications will be country-dependent.
KDIGO 2024 CLINICAL PRACTICE GUIDELINE FOR THE EVALUATION AND MANAGEMENT OF CHRONIC KIDNEY DISEASE S218
Recommendation 3.8.1: We suggest a nonsteroidal mineralocorticoid receptor antagonist with proven kidney or cardiovascular benefit for adults with T2D, an eGFR >25 ml/min per 1.73 m2 , normal serum potassium concentration, and albuminuria (>30 mg/g [>3 mg/mmol]) despite maximum tolerated dose of RAS inhibitor (RASi) (2A).
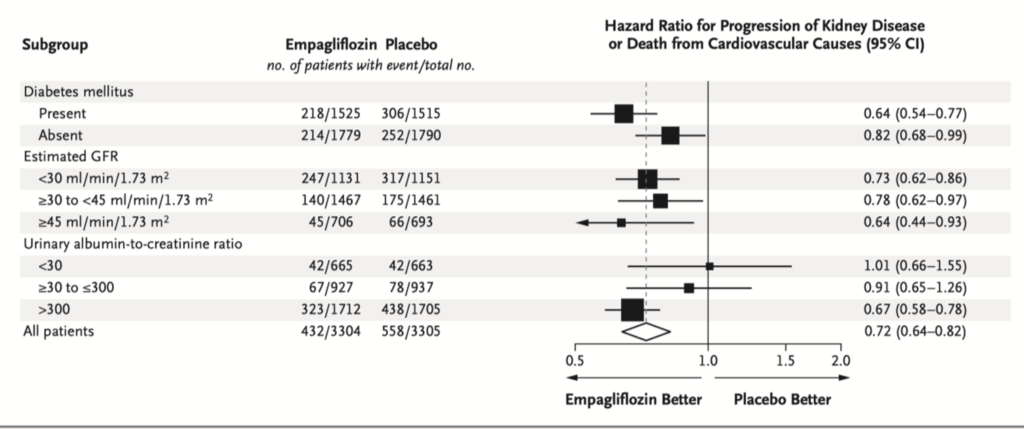
Recommendation 3.9.1: In adults with T2D and CKD who have not achieved individualized glycemic targets despite use of metformin and SGLT2 inhibitor treatment, or who are unable to use those medications, we recommend a long-acting GLP-1 RA (1B).
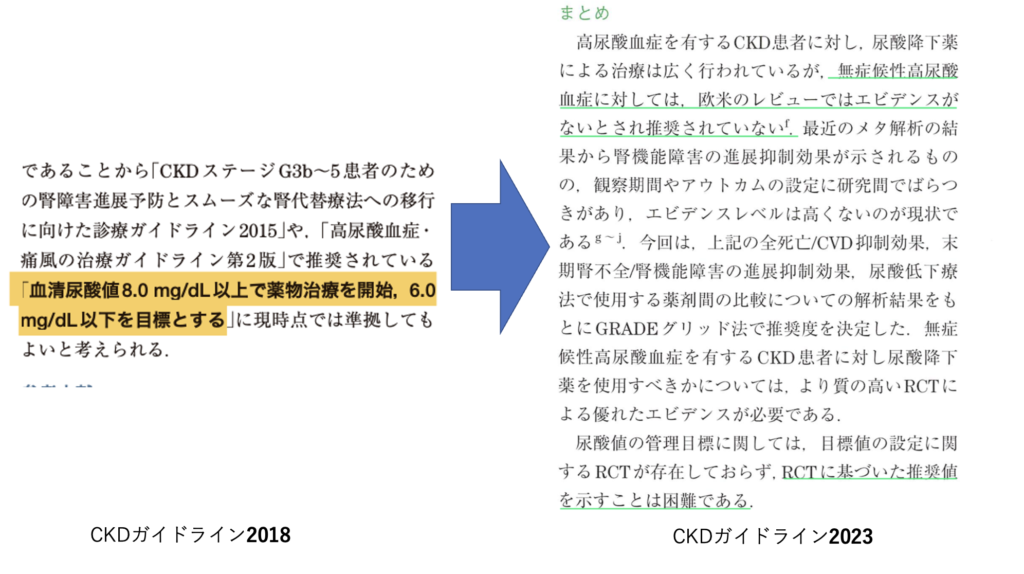
Recommendation 3.14.2: We suggest not using agents to lower serum uric acid in people with CKD and asymptomatic hyperuricemia to delay CKD progression (2D).
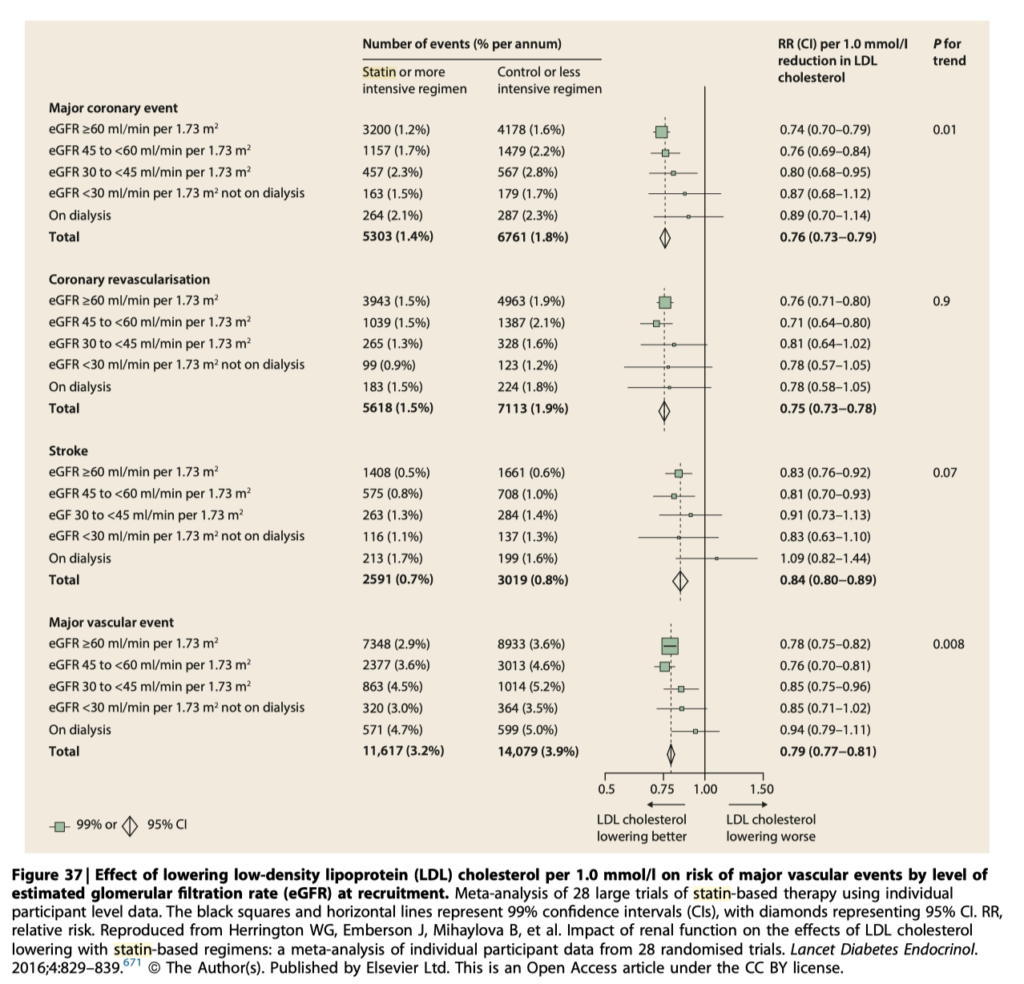
Recommendation 3.15.1.1: In adults aged ≧50 years with eGFR <60 ml/min per 1.73 m 2 but not treated with chronic dialysis or kidney transplantation (GFR categories G3a–G5), we recommend treatment with a statin or statin/ezetimibe combination (1A).
Recommendation 3.15.1.2: In adults aged ≧50 years with CKD and eGFR ≧60 ml/min per 1.73 m 2 (GFR categories G1–G2), we recommend treatment with a statin (1B).
CKD患者さんにはスタチンとエゼチミブを入れよう!という推奨です。
腎臓内科外来に来てる人、ほとんどが50歳以上ですからね。ほぼみんな適応になるレベルです。
透析患者さんには予後改善効果が低め。 KDIGO 2024 CLINICAL PRACTICE GUIDELINE FOR THE EVALUATION AND MANAGEMENT OF CHRONIC KIDNEY DISEASE
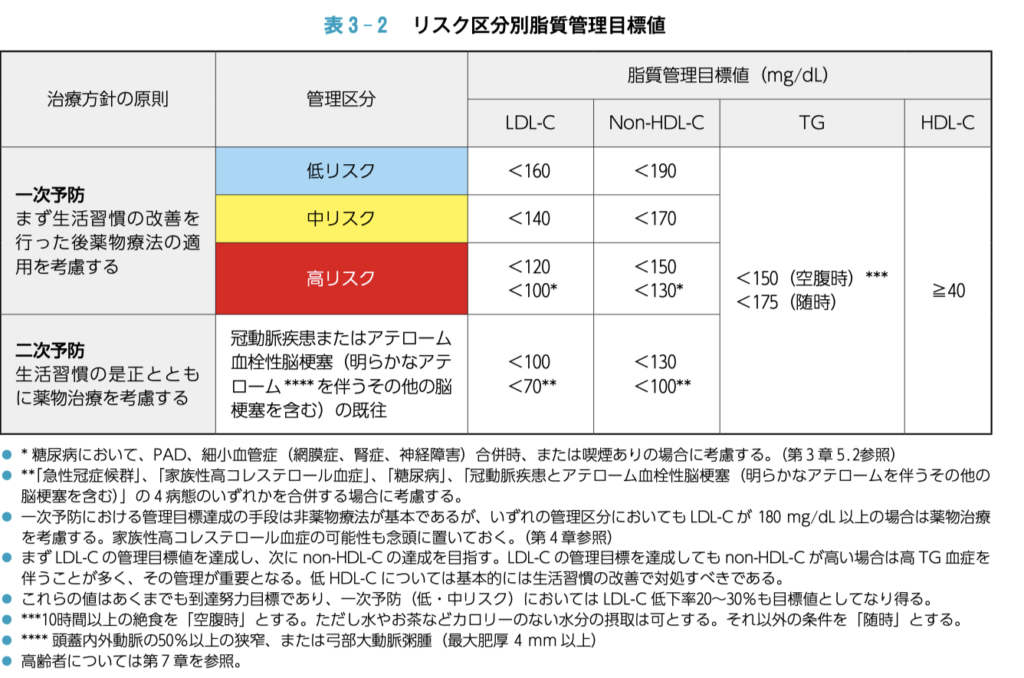
2022年の動脈硬化性疾患予防ガイドラインでも「Lower the better」の可能性は言及されていますが、頭蓋内出血のリスクが増えるかもとの記載もありますし、あくまでガイドラインの管理目標値以内を目指すでよいかと思います。

 専攻医
専攻医
 おちば
おちば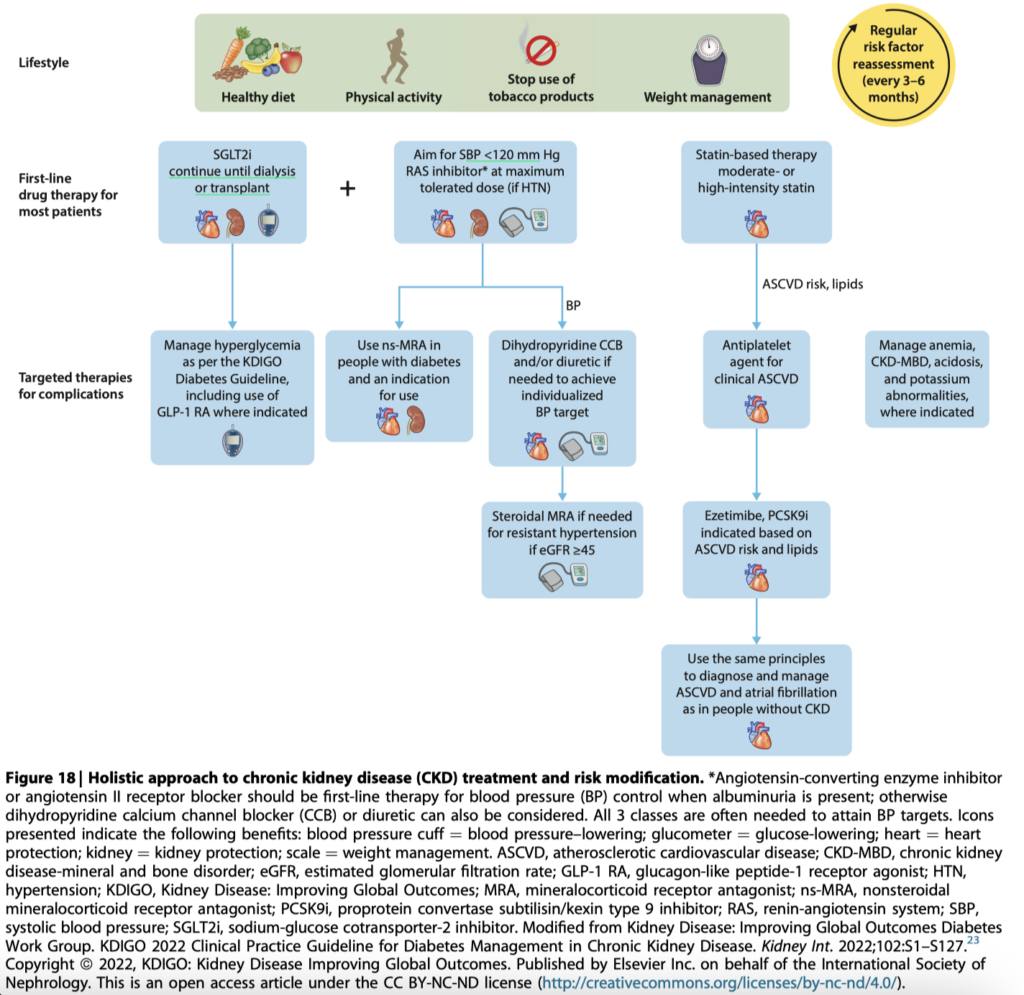
 KDIGOの中の人
KDIGOの中の人



コメント